

No One Need Allow Themselves to Be Fooled for a Second Time

Guy Hatchard
Many subscribers have requested an article specifically suitable for circulation to people in New Zealand who are beginning to question the official Covid narrative, but are still being bombarded by potentially misleading information. The following article has been written especially for this purpose, setting out the issues clearly and in historical order. It is sourced from official data and contains links with supplementary information. Please circulate widely to those feeling in need of answers.
This article is also available as a PDF to download, print, and/or share.
Newsroom is an independent news outlet which says it believes New Zealanders deserve exclusive, trustworthy, high quality independent local journalism. With this brief, we were astonished to read their article on Friday 6th September, entitled: The truth about New Zealand’s death rate that the Covid Commission will hear. It claimed that:
“Wild claims of excess deaths in the wake of the Covid vaccination campaign are at stark odds with the mathematical facts: New Zealand’s mortality rate is actually lower than expected.”
In other words, the article claims to have evidence that since the pandemic began no one has died from Covid infection or Covid vaccines who wouldn’t otherwise have died from other natural causes. The article was written by David Hood who is credited as an adviser for IT training and development at the University of Otago. Apparently, he is training us to believe that nothing extraordinary happened during the pandemic. Are they about to gaslight us again?
The article makes the outrageous claim that it is “demonstrably false” to say that New Zealand has had excess deaths in recent years. According to the article, people who claim that excess deaths have increased are not taking into account our rising total population and the fact that the population is ageing. The Newsroom piece is not a scientific article, it would not qualify for publication in a journal. It appears to be intended to influence public opinion. As the article dives into the statistics we quickly see that it appears to be employing a statistical sleight of hand that it is accusing others of using.
Age standardised adjustment of mortality data
The article tells us “New Zealand has seen big changes in ages, with 23 percent more living people aged 65-plus now than there were in 2017, as the children of the ‘£10 Pom’ migration era reach old age.” To the uninitiated, a 23% rise sounds huge, but in fact the figure is exaggerated and distorted by the author’s failure to take account of our rising population. In 2017 15% of the population were over 65, in 2023 16.6% of our population were over 65. That is a 10.5% rise over 6 years, not 23%.
The author correctly states that old people are more likely to die than young people, but the more than faint implication of the article was that somehow deaths of people over 65 don’t matter as much. In fact, statistics show the average kiwi should expect to live around 82 years. Below this age, your chances of dying decrease markedly. A 70 year old man in the USA for example has only a 2% chance of dying within 12 months.
The article suggests that if you take into account an ageing population, excess deaths disappear. Is this true? No, our article will explain why. So-called age standardisation of data is a complicated process. Current New Zealand population data ultimately references the census held in 2018. Every year there are hundreds of thousands people arriving or leaving New Zealand permanently with a range of ages. People die and are born, although continuously updated, gradually the data becomes less reliable.
In fact, broad adjustments based on large age ranges, such as the 60+ used in the graphics in the Newsroom article, actually mask the effect of the wide distribution of ages within any broad range. In New Zealand for example, the relative size of the most vulnerable 85+ years cohort with the highest death rate has remained unchanged since 2017. It has not increased. They made up 1.8% of the population then, and the exact same proportion in 2023. So is the author suggesting that the excess deaths are concentrated in the lower end of the 65+ age range? If he is, it is very concerning.
Due to the incidence of seasonal influenza, death rates vary slightly from year to year depending on the severity of the flu variant, but even so during the ten pre-pandemic years 2010 to 2019, New Zealand’s average rate of death was fairly consistent at 6.8 deaths per thousand population. During this time the 65+ cohort of the population rose by a significant 18%, but the death rate remained stable. It was 6.9 deaths per thousand in 2011 and 6.9 in 2019 for example. This is because survival rates for our biggest killers, cancer and heart disease, have been gradually improving which is exactly balancing out the effect of ageing on mortality. Therefore artificially subtracting deaths from mortality data based on minor and very gradual changes in age distribution, as the article suggests, is very problematic from a statistical point of view.
Excess deaths in New Zealand
So let’s look in detail at how the Hatchard Report has consistently and rigorously demonstrated that excess deaths in New Zealand during the pandemic are concerning. In 2020, New Zealand virtually closed its borders and quarantined the small number of arrivals. This continued until late 2021. Social distancing was encouraged and the health department tracked and traced the very small number of Covid cases. To all intents and purposes, New Zealand was Covid free. As a result, for the most part, we avoided the more deadly Alpha and Delta Covid variants. Something else happened, the closure of the borders meant that in 2020 and 2021 there were minimal cases of influenza type respiratory illness. In 2020 the mortality rate fell to just 6.4 deaths per thousand population, certainly the lowest for ten years, and probably the lowest ever. This was a very good outcome. There were 2000 fewer deaths in 2020 than would have been expected from the trend over the previous ten years. Well done New Zealand. We avoided the peak Covid deaths seen overseas.
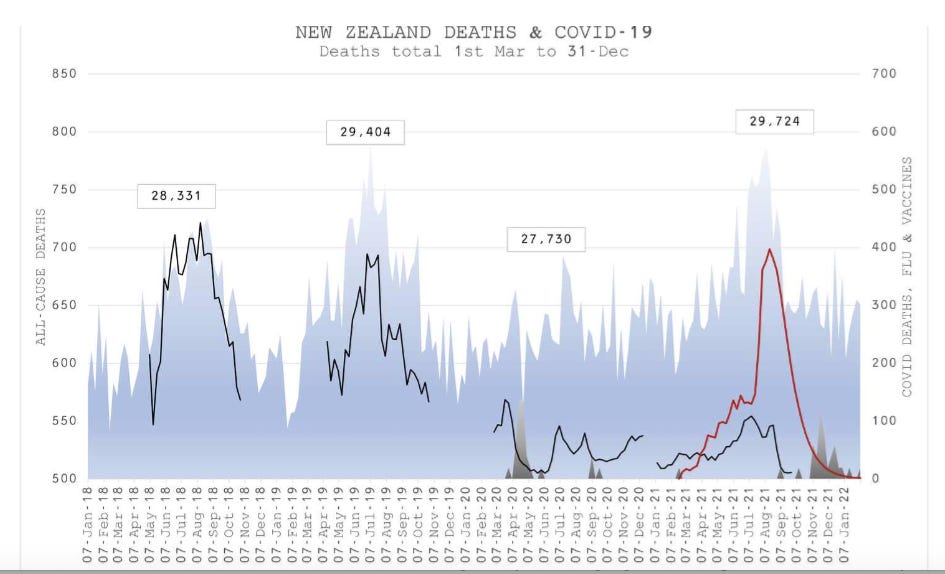
In 2021 we continued to be Covid free up until the year was drawing to a close. We were also largely influenza free. In March the mRNA Covid vaccination rollout began and something strange happened. The Hatchard Report reprinted the relevant weekly statistics in a single chart as above.
The shaded blue area represents all-cause deaths. The black line flu incidence. The shaded grey area Covid deaths. And the red line Covid vaccines administered. You can see very clearly that all cause mortality rose and peaked in line with Covid vaccinations despite the fact that there was virtually no Covid and very little influenza incidence. It is hard to escape the notion that Covid vaccines may have been causing an increase in mortality.
So what were people dying of? In February 2022 we reviewed the St John’s Ambulance call out data for 2021 which shed light on what was going on.
There were over 13 thousand additional callouts for chest pain, breathing problems, stroke and cardiac issues when compared to 2020 and the rise was not due to Covid or influenza. This also corresponded with tens of thousands of reports of similar vaccine injuries made to Medsafe by the end of 2021. Figures which Medsafe itself admits were vastly under reported.
New Zealand’s data was unique because unlike overseas, where Covid incidence and mortality was conflating any possible measurement of the effect of the Covid vaccines, we had an increase in death rates prior to Covid infection and in the absence of influenza, but after the introduction of Covid vaccines.
In early 2021 the Pfizer mRNA Covid vaccine rollout began. It was administered to approximately 90% of the adult New Zealand population. This was a novel type of biotech vaccine. Its mechanism was completely different from previous vaccines. To assess the effect of such an intervention the correct statistical methods to use are:
Assess the timeline of mortality rate and disease incidence before and after the intervention.
Assess any difference between the longer term trend before and after the intervention.
Assess any difference in mortality rates and disease incidence between those who were administered the intervention and those who were not.
With these definitive assessments you can judge if there is any evidence for a causal relationship between the jabs and mortality or disease rates.

We published this figure in 2022 compiled from official data being released weekly by Health New Zealand. It shows that any protective effect of the mRNA Covid vaccine wears off rapidly leaving the recipient with an immune deficit. A fact widely recognised in the published scientific data, and referenced in our recent “
Is Covid vaccination also making people sick?
We have discussed mortality figures, is there more to know?. In April 2023 we published
We have all been misled
People discussing these issues openly have been gaslit. The Newsroom article for example attempts to label those asking questions as outsiders with weird ideas. Nothing could be further from the truth. We are the ones talking common sense:
We all know what a vaccine is supposed to do, it should prevent disease. It is obvious to everyone now—even repeated Covid mRNA vaccines do not prevent Covid infection.
We also know that open government is a cornerstone of democracy, ours is anything but. It is hiding the concerning statistics.
The government signed a secret agreement granting Pzifer immunity from prosecution if there were adverse effects of mRNA Covid vaccines. Why did it do this for a novel untried medical intervention?
We know that looking for independent verification of results is an essential part of uncovering scientific truth. We were told not to go there. In order to save its own skin, our politicians and media have been describing this ordinary process of scientific investigation as a dangerous ‘rabbit hole’.
Mark Zuckerberg, CEO of Facebook, has admitted that the Biden administration pressured him into censoring Covid content. Similar censorship happened here in New Zealand. In 2021 we published a snapshot of Covid statistics on YouTube (owned by Google). This simply referenced New Zealand government sources. It was taken down by YouTube after 20,000 views within a matter of hours along with an advisory to us that Health New Zealand had required them to do so.
Health New Zealand failed to acknowledge the extent of the myocarditis risk among children and younger adults, ignoring for example definitive prospective studies such this preprint prospective study from Thailand which found that 29% of adolescents suffered cardiac irregularities after their second jab.
Health New Zealand failed to acknowledge that the three month long trials of Covid mRNA vaccines were poorly designed and gave no indication of the long term effects. Moreover, the trials assumed that adverse effects would be confined to a limited range of previously recognised effects of traditional vaccines, rather than the broad range, including cancers, heart disease, neurological and immune diseases predicted by a number of eminent researchers as likely additional outcomes of mRNA vaccination.
Our General Medical Council censored and even deregistered doctors warning their patients about potential side effects of Covid vaccines.
We now know that Health New Zealand secretly granted as many as 11,000 Covid vaccine exemptions to medical staff who knew enough about the risks to wish to avoid the jabs, but mostly refused exemptions for members of the public, even if they had medical conditions or a history that put them at risk of adverse effects of vaccination.
The Labour Government funded the media, in a successful attempt to influence their Covid content to align with government directives.
The Prime Minister’s Office funded a Disinformation Project with a specific remit to discredit anyone claiming a laboratory origin of Covid, mentioning herd immunity, or discussing the idea that some people might be dying ‘with Covid’, not ‘because’ of it.
Just remember, it is now clear and admitted by reputable mainstream media and government sources overseas that Covid escaped from a laboratory conducting gain of function research. So both Covid and Covid vaccines were the product of unregulated biotechnology. The vaccinated and unvaccinated have been pitted against one another by the media and the government in a cynical attempt to confuse the fundamental truth that our health has been damaged by biotechnology experimentation. This has prevented us all from taking common cause to call for open debate on biotechnology safety. New Zealand is almost alone among nations in continuing to maintain Covid vaccines are safe and effective. The article in Newsroom claims that the Covid Commission will hear the truth about excess deaths. I hope that they will.
Finally and crucially, why is our present National coalition government now proposing to deregulate biotechnology experimentation in the wake of the devastating pandemic death and sickness rates linked to biotechnology? This is incomprehensible and fraught with peril. It affects us all. We need to protect ourselves from this second wave of misinformation. The Hatchard Report has debunked the government biotech deregulation PR claims under the title “Fact Checking the Incredible Claims of Prime Minister Chris Luxon, Judith Collins and the New Zealand Biotech Lobby“. The implications for our food supply are explained in this article “Urgent: Government Plans To Remove Gene Food Labelling. We can also understand the hidden motivations and obvious drawbacks of biotech medicine by reading this article “The Government of the Bio-Technocrats“.